22
GUNAIKEIA
VOL 18 Nr 7
2013
De
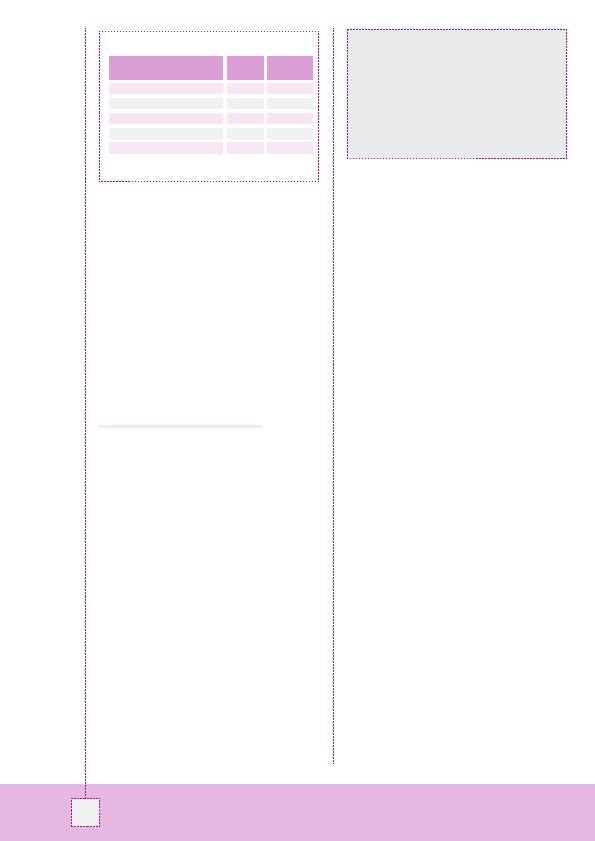
tabel vat de waarde van die screening samen. In te-
genstelling tot de eerste fase (jaarlijkse screening), waarin
alle kankers echografisch werden gediagnosticeerd, is een
bepaling van de CA125-spiegel in de tweede fase even
nuttig gebleken. Intervalkankers tot slot werden zeer snel
gediagnosticeerd.
De overleving tot slot was 91,9 maanden als de diagnose
werd gesteld minder dan één jaar na de laatste screening en
48,8 maanden als de diagnose werd gesteld meer dan één
jaar na de laatste screening (p = 0,037).
"Voorzichtigheid
is geboden bij de interpretatie van die resultaten aangezien
het geen gerandomiseerde studie is", commentarieerde
Rosenthal.
Endometriumkanker: denken aan
syndroom van lynch
"Het syndroom van Lynch is een hereditaire vatbaarheid
voor ontwikkeling van kanker van het colon, het endome-
trium, de ovaria, de maag, de dunne darm, de lever, de hoge
urinewegen, de hersenen en de huid", zei Sarah Ferguson
(toronto). Het risico op endometriumkanker bedraagt 30-
60% (tegen `slechts' 2% in de algemene bevolking). Het
syndroom wordt overigens vaak gediagnosticeerd naar
aanleiding van endometriumkanker en daarom is een spe-
cifieke screening gewettigd om tijdig een tweede kanker te
kunnen opsporen en de impact ervan te verminderen (26).
Maar wat is de beste screeningstrategie? Om dat na te
gaan heeft de groep van toronto een prospectieve studie
uitgevoerd bij alle vrouwen met een histologisch bewe-
zen endometriumkanker in hun centrum (n = 118). Bij een
groot aantal van die vrouwen was de familiale geschiede-
nis verdacht (n = 25) (27). Er werd een genetisch onder-
zoek uitgevoerd gekoppeld aan een biologische analyse
van de tumor en een analyse van de kenmerken van de
endometriumkanker bij het syndroom van lynch (infiltra-
tie van lymfocyten in en rond de tumor, heterogene tumor,
preferentiële ligging in het onderste segment, mucineuze
differentiatie). Op die manier kon bij 17% van de patiënten
een syndroom van lynch worden vermoed. tevens kon zo
worden aangetoond dat familiale antecedenten niet vol-
doende discriminerend zijn en dat de morfologische ken-
merken van de kanker geen efficiënte screening strategie
mogelijk maken, in tegenstelling tot de immunohistoche-
mie. En dat
"vooral bij vrouwen jonger dan 60 jaar. Alle
vrouwen met een verdachte familiale voorgeschiedenis
moeten worden onderzocht", concludeerde ze.
Referenties
1.
Kehoe S, Hook J, Nankivell M, et al. Chemotherapy or upfront surgery for newly
diagnosed advanced ovarian cancer: results from the MrC CHOrUS trial. ASCO 2013.
Abstract#5500.
2.
rose PG, Brady MF. EOrtC 55971: does it apply to all patients with advanced state
ovarian cancer? Gynecol Oncol 2011;120(2):300-1.
3.
Katsumata N, Yasuda M, takahashi F, et al. Dose-dense paclitaxel once a week in
combination with carboplatin every 3 weeks for advanced ovarian cancer: a phase 3,
open-label, randomised controlled trial. lancet 2009;374(9698):1331-8.
4.
Pignata S, Scambia G, lauria r, et al. A randomized multicenter phase III study comparing
weekly versus every 3 weeks carboplatin (C) plus paclitaxel (P) in patients with advanced
ovarian cancer (AOC): Multicenter Italian trials in Ovarian Cancer (MItO-7--European
Network of Gynaecological Oncological trial Groups (ENGOt-ov-10) and Gynecologic
Cancer Intergroup (GCIG) trial. ASCO 2013. Abstract#lBA5501.
5.
Cervantes-ruiperez A, Hoskins P, Vergote I, et al. Final results of OV16, a phase III
randomized study of sequential cisplatin-topotecan and carboplatin-paclitaxel (CP) versus
CP in first-line chemotherapy for advanced epithelial ovarian cancer (EOC): A GCIG study
of NCIC CtG, EOrtC-GCG, and GEICO. ASCO 2013. Abstract#5502.
6.
Hoskins P, Vergote I, Cervantes A, et al. Advanced ovarian cancer: phase III randomized
study of sequential cisplatin-topotecan and carboplatin-paclitaxel vs carboplatin-
paclitaxel. J Natl Cancer Inst 2010;102(20):1547-56.
7.
Friedlander M, Hancock KC, rischin D, et al. A Phase II, open-label study evaluating
pazopanib in patients with recurrent ovarian cancer. Gynecol Oncol 2010;119(1):32-7.
8.
Du Bois A, Floquet A, Kim J, et al. randomized, double-blind, phase III trial of pazopanib
versus placebo in women who have not progressed after first-line chemotherapy for
advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer (AEOC): results
of an international Intergroup trial (AGO-OVAr16). ASCO 2013. Abstract#lBA5503.
9.
Cancer Genome Atlas research Network. Integrated genomic analyses of ovarian
carcinoma. Nature 2011;474(7353):609-15.
10. Degenhardt Y, lampkin t. targeting Polo-like kinase in cancer therapy. Clin Cancer res
2010;16(2):384-9.
11. rudolph D, Steegmaier M, Hoffmann M, et al. BI 6727, a Polo-like kinase inhibitor
with improved pharmacokinetic profile and broad antitumor activity. Clin Cancer res
2009;15(9):3094-102.
12. Schöffski P, Awada A, Dumez H, et al. A phase I, dose-escalation study of the novel Polo-
like kinase inhibitor volasertib (BI 6727) in patients with advanced solid tumours. Eur J
Cancer 2012;48(2):179-86.
13. Pujade-lauraine E, Weber B, ray-Coquard I, et al. Phase II trial of volasertib (BI 6727)
versus chemotherapy (Ct) in platinum-resistant/refractory ovarian cancer (OC). ASCO
2013. Abstract#5505.
14. Bast rC Jr, Hennessy B, Mills GB. the biology of ovarian cancer: new opportunities for
translation. Nat rev Cancer 2009;9(6):415-28.
15. Press JZ, De luca A, Boyd N, et al. Ovarian carcinomas with genetic and epigenetic BrCA1
loss have distinct molecular abnormalities. BMC Cancer 2008;8:17. doi: 10.1186/1471-
2407-8-17.
16. Gelmon KA, tischkowitz M, Mackay H, et al. Olaparib in patients with recurrent high-
grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer:
a phase 2, multicentre, open-label, non-randomised study.
lancet Oncol 2011;12(9):852-61.
17. ledermann J, Harter P, Gourley C, et al. Olaparib maintenance therapy in platinum-
sensitive relapsed ovarian cancer. N Engl J Med 2012;366(15):1382-92.
18. ledermann J, Harter P, Gourley C, et al. Olaparib maintenance therapy in patients with
platinum-sensitive relapsed serous ovarian cancer (SOC) and a BrCA mutation (BrCAm).
ASCO 2013. Abstract#5505.
19. Noda K, Ohashi Y, Okada H, et al. randomized phase II study of immunomodulator
Z-100 in patients with stage IIIB cervical cancer with radiation therapy. Jpn J Clin Oncol
2006;36(9):570-7.
20. Noda K, Ohashi Y, Sugimori H, et al. Phase III double-blind randomized trial of radiation
therapy for stage IIIb cervical cancer in combination with low- or high-dose Z-100:
treatment with immunomodulator, more is not better. Gynecol Oncol 2006;101(3):455-63.
21. Fujiwara K, Ohashi Y, Ochiai K, Noda K. Phase III placebo controlled double blind
randomized trial of radiation therapy for stage 2B-4A cervical cancer with
immunomodulator Z-100: JGOG-Dt101 study. ASCO 2013. Abstract#5506.
22. Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-t immunotherapy for castration-
resistant prostate cancer. N Engl J Med 2010;363(5):411-22.
23. Hogg r, Friedlander M. Biology of epithelial ovarian cancer: implications for screening
women at high genetic risk. J Clin Oncol 2004;22(7):1315-27.
24. rosenthal AN, Fraser l, Manchanda r, et al. results of annual screening in phase I of
the United Kingdom familial ovarian cancer screening study highlight the need for strict
adherence to screening schedule. J Clin Oncol 2013;31(1):49-57.
25. rosenthal A, Fraser l, Philpott S, et al. Final results of 4-monthly screening in the UK
Familial Ovarian Cancer Screening Study (UKFOCSS Phase 2). ASCO 2013. Abstract#5507^.
26. Hampel H, Frankel W, Panescu J, et al. Screening for lynch syndrome (hereditary
nonpolyposis colorectal cancer) among endometrial cancer patients. Cancer res
2006;66(15):7810-7.
27. Ferguson S. Screening for lynch syndrome in unselected women with endometrial cancer.
ASCO 2013. Abstract#5508.
Tabel: Waarde van intensieve screening.
Kenmerk
Waarde
(%)
95%CI
Sensitiviteit (occult echt pos.)
100.0
73.5-100
Sensitiviteit (occult vals neg.)
75.0
47.6-92.7
Specificiteit (occult n/a)
96.1
95.2-97.0
PPV (occult vals neg.)
13.0*
6.9-21.7
NPV (occult vals neg.)
99.7
99.3-99.9
* Vergeleken met 25% in fase I
"Het is niet zozeer door vaak de CA125-spiegel te bepalen,
maar wel door een strikte naleving van het (weliswaar
jaarlijkse) protocol dat het risico het best kan worden verlaagd.
Wat de conclusie van Sarah Ferguson betreft, we zouden die
nog moeten confronteren met de economische realiteit met
inbegrip van de familiale gevolgen. En die berekening blijkt
positief te zijn met gerichte immunohistochemie, althans bij
vrouwen jonger dan 60 jaar."
Michael Friedlander (Sidney)