ben dat een palliatieve androgeen-
deprivatie vroeger wordt ingesteld bij
een minimale asymptomatische ziek-
te, aangezien er geen overlevingsvoor-
deel is vastgesteld bij het vroeg starten
van deze therapie (25). Er dient echter
wel rekening gehouden te worden met
een belangrijke lead time bias bij het
interpreteren van de eindpunten over
gerichte therapie van oligometastasen.
Hierbij worden metastasen vaak actief
opgespoord, in tegenstelling tot histo-
rische studies waarbij er niet gescreend
werd voor metastasen. Bovendien zijn
er geen studies die de natuurlijke pro-
gressie (zonder therapie) van oligome-
tastasen in kaart hebben gebracht. Op
dit moment is het dus niet zeker dat
een gerichte therapie van metastasen
bij PK het ziekteverloop verandert.
bieden, werd er recent een gerandomi-
seerde fase 2-studie opgestart in het
UZ Gent, waarbij patiënten met oligo-
metastasen gerandomiseerd worden
tussen een gerichte behandeling van
de metastasen en een actieve opvol-
ging (clinicaltrials.gov: NCT01558427).
uitstellen van een palliatieve AD.
dat een niet-systemische behandeling
voor beperkte metastasen van PK veilig
kan, zowel met heelkunde als radiothe-
rapie als met een tijdelijke biochemische
en klinische respons. Toch moet deze be-
handelingsstrategie, gezien het beperkte
aantal patiënten die op deze manier be-
handeld werden, de korte opvolging en
het ontbreken van een controlegroep als
experimenteel beschouwd te worden en
te gebeuren binnen studieverband.
1.
cancer incidence and mortality in Europe in 2008. Eur J
Cancer. 2010;46(4):765781.
prostate cancer. Part II: Treatment of advanced, relapsing,
and castration-resistant prostate cancer. Eur. Urol.
2011;59(4):572583.
effects of androgen-deprivation therapy in men with
prostate cancer. Cancer. 2009;115(11):23882399.
and survival in hormonally treated metastatic prostate
cancer. Int. J. Urol. 1999;6(5):240244.
History of Noncastrate Metastatic Prostate Cancer after
Radical Prostatectomy. Eur. Urol. 2007;51(4):940948.
represent a significant cut-off value for cancer specific
survival in patients with node positive prostate cancer.
A new proposal based on a two-institution experience
on 703 consecutive N+ patients treated with radical
prostatectomy, extended pelvic lymph node dissection
and adjuvant therapy. Eur. Urol. 2009;55(2):261270.
subset of patients with prostate cancer who develop
oligometastases? Int J Radiat Oncol Biol Phys.
2004;58(1):310.
Oncol. 1995;13(1):810.
radiotherapy for multisite extracranial oligometastases: final
report of a dose escalation trial in patients with 1 to 5 sites of
metastatic disease. Cancer. 2012;118(11):29622970.
2007;30(6):637644.
prostatectomy. JAMA. 1999;281(17):15911597.
for post-prostatectomy biochemical recurrence. Clin
Oncol (R Coll Radiol). 2010;22(1):4655.
Medicine. 2011;52(1):8189.
in the management of patients with prostate-specific
antigen progression after radical treatment of prostate
cancer. Eur. Urol. 2011;59(1):5160.
prostate cancer patients with biochemical failure after
radical prostatectomy. Eur J Nucl Med Mol Imaging.
2010;37(6):11061116.
radical prostatectomy with biochemical recurrence and
nodal recurrence detected by [11C]choline positron
emission tomography/computed tomography. Eur. Urol.
2011;60(5):935943.
in patients with PSA failure and single lymph node
recurrence after radical retropubic prostatectomy. Urol
Int. 2010;84(4):418423.
recurrence after radical prostatectomy. World J Urol.
2009;27(5):619625.
tomography-positive lymph nodes in patients with
biochemical failure after treatment for localized prostate
cancer. BJU International. 2008;102(4):446451.
with PSA Failure after Radical Prostatectomy: Lessons
Learned from Eight Cases. Adv Urol. 2012;2012:601572.
detected with choline PET scan in prostate cancer
patients. Tumori. 2011;97(1):4955.
bone metastases of prostate cancer. Urol. Oncol. 2011;
for isolated lymph node recurrent prostate cancer.
Radiother Oncol. 2009;93(1):1417.
limited prostate cancer metastases: deferring androgen
deprivation therapy. Clin Gentourin Cancer. 2012. In Press.
The Medical Research Council Prostate Cancer Working
Party Investigators Group. Br J Urol. 1997;79(2):235246.
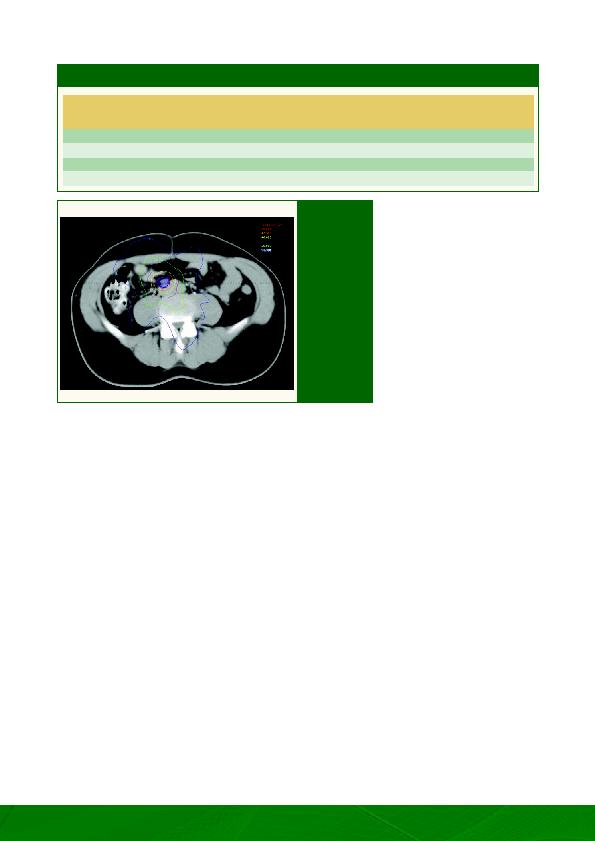
snede van een
behandelingsplan
met de verschil-
lende isodosen
voor een lymfe-
kliermetastase
ter hoogte van de
iliaca communis.
De voorgeschre-
ven dosis bedraagt
50 Gray in 10
fracties. Het doel-
volume, afgebeeld
in donkerblauw,
bestaat uit de ver-
grote klier met een
veiligheidsmarge
van 3mm.