8
GUNAIKEIA
VOL 18 N°9
2013
Traitement
Même si le traitement se veut aussi conservateur que
possible, on opte souvent pour une chirurgie radicale
(
Figure 2), laquelle peut être associée à une morbidité supé-
rieure (2, 5-7). Cette intervention s'accompagne de saigne-
ments très abondants et requiert assurément un contrôle
peropératoire et post-opératoire (2). Toutefois, si la patiente
exprime un désir de grossesse ou qu'une morbidité élevée
est à prévoir, l'intervention chirurgicale est moins radicale
(2). Heureusement, la présence de la tumeur n'engage pas
en soi le pronostic vital. Aussi, on peut se permettre de ne
réaliser qu'une résection partielle. Chez les patientes subis-
sant une exérèse partielle, un suivi à long terme et une large
résection en cas de récidive locale sont essentiels (21). En
cas de résection incomplète ou de récidive, on opte pour
l'hormonothérapie. Pour cela, il faut que la tumeur soit hor-
monosensible. Le cas échéant, on utilise un agoniste de la
GnRH, du tamoxifène ou du raloxifène. Ces médicaments
peuvent servir à réduire le volume tumoral, de manière à
pouvoir réséquer complètement les grosses tumeurs (2,
7). Des travaux d'étude récents montrent qu'il n'y a aucun
avantage à réséquer la tumeur avec une plus grande marge.
Ainsi, le nombre de rechutes rapporté chez les patientes
avec des marges de résection négatives était pratique-
ment similaire à celui enregistré chez les patientes avec des
marges positives (5). La récidive peut avoir lieu de quelques
mois à 20 ans après l'opération (7). La chimiothérapie et la
radiothérapie ne sont pas recommandées. La chimio-em-
bolisation peut parfois être utile pour réduire le volume
tumoral et permettre ainsi une résection plus complète (8).
Compte tenu du taux de récurrence élevé (30-72%), un suivi
et un contrôle à long terme sont nécessaires, même en cas
de marges de résection négatives (2, 5). Un examen clinique
périodique ne suffit pas pour diagnostiquer une rechute en
temps opportun. Pour déceler une rechute à un stade pré-
coce, l'imagerie (IRM, par ex.) est indispensable.
Conclusion
L'AMA est une tumeur mésenchymateuse myxoïde rare
qui se développe essentiellement au niveau du bassin et
du périnée de femmes se trouvant dans la période de re-
production. La plupart du temps, il ne métastase pas. La
tumeur peut envahir les structures avoisinantes, mais se li-
mite généralement à faire pression dessus. Une caractéris-
tique typique de l'AMA réside dans sa tendance à récidiver
localement. Dès lors, un traitement radical efficace, avec
résection complète et hormonothérapie (en cas de tumeur
hormonodépendante), est indispensable. Un suivi intensif
est nécessaire, dans la mesure où la tumeur peut récidi-
ver dans un délai allant de quelques mois à 20 ans après
l'opération. La maladie étant souvent mal diagnostiquée, il
convient de redoubler d'attention en présence d'une masse
vulvaire. Nous devons poursuivre les recherches sur le rôle
du CD44, du CD34 et de HMGI-C en tant que marqueurs
tumoraux. Des directives doivent impérativement être défi-
nies pour le traitement.
Références
1.
Steeper TA, Rosai J. Aggressive angiomyxoma of the female pelvis and perineum. Report
of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am J Surg Pathol
1983;7(5):463-75. PubMed PMID: 6684403. Epub 1983/07/01. eng.
2.
Dierickx I, Deraedt K, Poppe W, Verguts J. Aggressive angiomyxoma of the vulva: a case
report and review of literature. Arch Gynecol Obstet 2008;277(6):483-7. PubMed PMID:
18214507.
3.
Barmon D, Kataki AC, Sharma JD, Bordoloi J. Aggressive angiomyxoma of the vulva.
Journal of mid-life health 2012;3(1):47-9. PubMed PMID: 22923982. Pubmed Central
PMCID: PMC3425151. Epub 2012/08/28. eng.
4.
Geng J, Cao B, Wang L. Aggressive angiomyxoma: an unusual presentation. Korean
journal of radiology: official journal of the Korean Radiological Society 2012;13(1):90-3.
PubMed PMID: 22247641. Pubmed Central PMCID: PMC3253408. Epub 2012/01/17. eng.
5.
Chan YM, Hon E, Ngai SW, Ng TY, Wong LC. Aggressive angiomyxoma in females: is radical
resection the only option? Acta Obstet Gynecol Scand 2000;79(3):216-20. PubMed PMID:
10716303. Epub 2000/03/15. eng.
6.
Ichinokawa Y, Sadamasa H, Hiruma M, et al. Case of aggressive angiomyxoma of the
vulva. J Dermatol 2012 Mar 27. PubMed PMID: 22452584. Epub 2012/03/29. Eng.
7.
Bagga R, Keepanasseril A, Suri V, Nijhawan R. Aggressive angiomyxoma of the vulva in
pregnancy: a case report and review of management options. MedGenMed : Medscape
general medicine. 2007;9(1):16. PubMed PMID: 17435625. Pubmed Central PMCID:
PMC1925027. Epub 2007/04/17. eng.
8.
Han-Geurts IJ, van Geel AN, van Doorn L, den Bakker M, Eggermont AM, Verhoef C.
Aggressive angiomyxoma: multimodality treatments can avoid mutilating surgery. Eur J
Surg Oncol 2006;32:1217-21.
9.
Srinivasan R, Mohapatra N, Malhotra S, Rao SK. Aggressive angiomyxoma presenting as a
vulval polyp. Indian journal of cancer. 2007 Apr-Jun;44(2):87-9. PubMed PMID: 17938485.
Epub 2007/10/17. eng.
10. Nucci MR, Weremowicz S, Neskey DM, et al. Chromosomal translocation t(8;12)
induces aberrant HMGIC expression in aggressive angiomyxoma of the vulva. Genes,
Chromosomes Cancer 2001;32(2):172-6. PubMed PMID: 11550285. Epub 2001/09/11. eng.
11. Menzel T, Fletcher CD. The emerging role of myofibroblasts in soft tissue neoplasia. Am J
Clin Pathol 1997;107(1):2-5. PubMed PMID: 8980359. Epub 1997/01/01. eng.
12. Silverman JS, Albukerk J, Tamsen A. Comparison of angiomyofibroblastoma and
aggressive angiomyxoma in both sexes: four cases composed of bimodal CD34 and factor
XIIIa positive dendritic cell subsets. Pathol Res Pract 1997;193(10):673-82. PubMed PMID:
9505259. Epub 1997/01/01. eng.
13. Fetsch JF, Laskin WB, Lefkowitz M, Kindblom LG, Meis-Kindblom JM. Aggressive
angiomyxoma: a clinicopathologic study of 29 female patients. Cancer 1996;78(1):79-90.
PubMed PMID: 8646730. Epub 1996/07/01. eng.
14. Amezcua CA, Begley SJ, Mata N, Felix JC, Ballard CA. Aggressive angiomyxoma of the
female genital tract: a clinicopathologic and immunohistochemical study of 12 cases.
International journal of gynecological cancer: official journal of the International
Gynecological Cancer Society 2005;15(1):140-5. PubMed PMID: 15670309. Epub
2005/01/27. eng.
15. Bigotti G, Coli A, Gasbarri A, Castagnola D, Madonna V, Bartolazzi A.
Angiomyofibroblastoma and aggressive angiomyxoma: two benign mesenchymal
neoplasms of the female genital tract. An immunohistochemical study. Pathol Res Pract
1999;195(1):39-44. PubMed PMID: 10048093. Epub 1999/02/27. eng.
16. Nalini G, Duggal R, Neelam A, Vanita S, Arvind R. Fine needle aspiration cytology in a case
of recurrent aggressive angiomyxoma of vulva. Cytopathology: official journal of the
British Society for Clinical Cytology 2010;21(3):207-8. PubMed PMID: 19843146. Epub
2009/10/22. eng.
17. Outwater EK, Marchetto BE, Wagner BJ, Siegelman ES. Aggressive angiomyxoma: findings
on CT and MR imaging. AJR American journal of roentgenology 1999;172(2):435-8.
PubMed PMID: 9930798. Epub 1999/02/04. eng.
18. Havel G, Burian P, Kohrtz M, Mark J. Aggressive angiomyxoma of the vulva: an unusual,
deceptive and recurrence-prone tumour with evidence of estrogen receptor expression.
Case report. APMIS: acta pathologica, microbiologica, et immunologica Scandinavica
1994;102(3):236-40. PubMed PMID: 8185891. Epub 1994/03/01. eng.
19. Htwe M, Deppisch LM, Saint-Julien JS. Hormone-dependent, aggressive angiomyxoma
of the vulva. Obstet Gynecol 1995;86(4 Pt 2):697-9. PubMed PMID: 7675419. Epub
1995/10/01. eng.
20. Zhang P, Song K, Li L, et al. Aggressive Angiomyxoma with massive ascites. Gynecologic
Oncology Case Reports 2011;1(1):12-3.
21. Gungor T, Zengeroglu S, Kaleli A, Kuzey GM. Aggressive angiomyxoma of the vulva
and vagina. A common problem: misdiagnosis. Eur J Obstet Gynecol Reprod Biol
2004;112(1):114-6. PubMed PMID: 14687754. Epub 2003/12/23. eng.
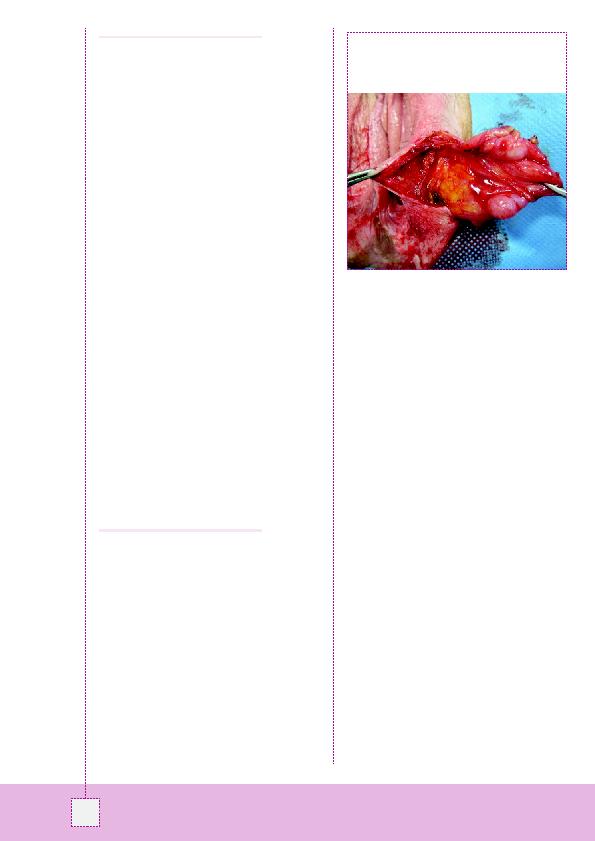
Figure 2: La masse lobulée a été réséquée en bloc avec le
tissu conjonctif adjacent. La masse s'étendait à la région
paraclitoridienne. L'examen au microscope a révélé que les
marges de résection étaient saines.