22
GUNAIKEIA
VOL 18 N°7
2013
Dernier point, «
à prendre cependant avec précaution car il
ne s'agissait pas d'une étude randomisée», précise Rosen-
thal, la survie a été de 91,9 mois lorsque le diagnostic a été
effectué moins d'un an après le dernier dépistage contre
48,8 mois lorsque le diagnostic a été réalisé plus d'un an
après le dernier dépistage (p = 0,037).
Cancer de l'endomètre: une sentinelle du
syndrome de Lynch
«
Le syndrome de Lynch est une susceptibilité héréditaire
de développer un cancer du côlon et un cancer de l'endo-
mètre, de l'ovaire, de l'estomac, de l'intestin grêle, du foie,
de l'appareil urinaire supérieur, du cerveau et de la peau»,
rappelle Sarah Ferguson (toronto). Pour le cancer de l'en-
domètre, ce risque est de 30-60%, alors qu'il n'est «que»
de 2% dans la population générale. il est par ailleurs sou-
vent un cancer «sentinelle» de ce syndrome et justifie donc
à ce titre un dépistage spécifique de manière à pouvoir
anticiper un second cancer et en diminuer l'impact (26).
Reste à savoir quelle est la meilleure stratégie de dépis-
tage, ce que l'équipe de Toronto a investigué de manière
prospective sur tous les cancers endométriaux histolo-
giquement confirmés dans son centre (n = 118) et dont
un grand nombre avait une histoire familiale suspecte
(n = 25) (27). Une recherche génétique a été effectuée,
couplée d'une part à une analyse biologique de la tumeur,
d'autre part à une analyse des caractéristiques propres au
cancer de l'endomètre du syndrome de Lynch (infiltration
lymphocytaire tumorale et péritumorale, hétérogénéité de
la tumeur, situation préférentielle dans le segment infé-
rieur, différenciation mucineuse). Ce travail a conduit à
suspecter un syndrome de Lynch dans 17% des cas et à
établir, d'une part, que l'histoire familiale n'est pas suffi-
samment discriminante et, d'autre part, que la morpho-
logie du cancer ne permet pas de stratégie efficace de
dépistage, contrairement à l'immunohistochimie. Et ce
«
particulièrement chez les femmes de moins de 60 ans, un
examen à réaliser chez toutes les femmes dont l'histoire
familiale est simplement suspecte», conclut-elle.
Références
1.
Kehoe S, Hook J, Nankivell M, et al. Chemotherapy or upfront surgery for newly
diagnosed advanced ovarian cancer: Results from the MRC CHORUS trial. ASCO 2013.
Abstract#5500.
2.
Rose PG, Brady MF. EORTC 55971: does it apply to all patients with advanced state
ovarian cancer? Gynecol Oncol 2011;120(2):300-1.
3.
Katsumata N, Yasuda M, Takahashi F, et al. Dose-dense paclitaxel once a week in
combination with carboplatin every 3 weeks for advanced ovarian cancer: a phase 3,
open-label, randomised controlled trial. Lancet 2009;374(9698):1331-8.
4.
Pignata S, Scambia G, Lauria R, et al. A randomized multicenter phase III study comparing
weekly versus every 3 weeks carboplatin (C) plus paclitaxel (P) in patients with advanced
ovarian cancer (AOC): Multicenter italian trials in Ovarian Cancer (MitO-7--European
Network of Gynaecological Oncological trial Groups (ENGOt-ov-10) and Gynecologic
Cancer Intergroup (GCIG) trial. ASCO 2013. Abstract#LBA5501.
5.
Cervantes-Ruiperez A, Hoskins P, Vergote I, et al. Final results of OV16, a phase III
randomized study of sequential cisplatin-topotecan and carboplatin-paclitaxel (CP) versus
CP in first-line chemotherapy for advanced epithelial ovarian cancer (EOC): A GCIG study
of NCIC CTG, EORTC-GCG, and GEICO. ASCO 2013. Abstract#5502.
6.
Hoskins P, Vergote I, Cervantes A, et al. Advanced ovarian cancer: phase III randomized
study of sequential cisplatin-topotecan and carboplatin-paclitaxel vs carboplatin-
paclitaxel. J Natl Cancer Inst 2010;102(20):1547-56.
7.
Friedlander M, Hancock KC, Rischin D, et al. A Phase II, open-label study evaluating
pazopanib in patients with recurrent ovarian cancer. Gynecol Oncol 2010;119(1):32-7.
8.
Du Bois A, Floquet A, Kim J, et al. Randomized, double-blind, phase III trial of pazopanib
versus placebo in women who have not progressed after first-line chemotherapy for
advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer (AEOC): Results
of an international Intergroup trial (AGO-OVAR16). ASCO 2013. Abstract#LBA5503.
9.
Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian
carcinoma. Nature 2011;474(7353):609-15.
10. Degenhardt Y, Lampkin T. Targeting Polo-like kinase in cancer therapy. Clin Cancer Res
2010;16(2):384-9.
11. Rudolph D, Steegmaier M, Hoffmann M, et al. BI 6727, a Polo-like kinase inhibitor
with improved pharmacokinetic profile and broad antitumor activity. Clin Cancer Res
2009;15(9):3094-102.
12. Schöffski P, Awada A, Dumez H, et al. A phase I, dose-escalation study of the novel Polo-
like kinase inhibitor volasertib (BI 6727) in patients with advanced solid tumours. Eur J
Cancer 2012;48(2):179-86.
13. Pujade-Lauraine E, Weber B, Ray-Coquard I, et al. Phase II trial of volasertib (BI 6727)
versus chemotherapy (CT) in platinum-resistant/refractory ovarian cancer (OC). ASCO
2013. Abstract#5505.
14. Bast RC Jr, Hennessy B, Mills GB. The biology of ovarian cancer: new opportunities for
translation. Nat Rev Cancer 2009;9(6):415-28.
15. Press JZ, De Luca A, Boyd N, et al. Ovarian carcinomas with genetic and epigenetic BRCA1
loss have distinct molecular abnormalities. BMC Cancer 2008;8:17. doi: 10.1186/1471-
2407-8-17.
16. Gelmon KA, Tischkowitz M, Mackay H, et al. Olaparib in patients with recurrent high-
grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer:
a phase 2, multicentre, open-label, non-randomised study. Lancet Oncol 2011;12(9):852-
61.
17. Ledermann J, Harter P, Gourley C, et al. Olaparib maintenance therapy in platinum-
sensitive relapsed ovarian cancer. N Engl J Med 2012;366(15):1382-92.
18. Ledermann J, Harter P, Gourley C, et al. Olaparib maintenance therapy in patients with
platinum-sensitive relapsed serous ovarian cancer (SOC) and a BRCA mutation (BRCAm).
ASCO 2013. Abstract#5505.
19. Noda K, Ohashi Y, Okada H, et al. Randomized phase II study of immunomodulator
Z-100 in patients with stage IIIB cervical cancer with radiation therapy. Jpn J Clin Oncol
2006;36(9):570-7.
20. Noda K, Ohashi Y, Sugimori H, et al. Phase III double-blind randomized trial of radiation
therapy for stage IIIb cervical cancer in combination with low- or high-dose Z-100:
treatment with immunomodulator, more is not better. Gynecol Oncol 2006;101(3):455-63.
21. Fujiwara K, Ohashi Y, Ochiai K, Noda K. Phase III placebo controlled double blind
randomized trial of radiation therapy for stage 2B-4A cervical cancer with
immunomodulator Z-100: JGOG-DT101 study. ASCO 2013. Abstract#5506.
22. Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-
resistant prostate cancer. N Engl J Med 2010;363(5):411-22.
23. Hogg R, Friedlander M. Biology of epithelial ovarian cancer: implications for screening
women at high genetic risk. J Clin Oncol 2004;22(7):1315-27.
24. Rosenthal AN, Fraser L, Manchanda R, et al. Results of annual screening in phase I of
the United Kingdom familial ovarian cancer screening study highlight the need for strict
adherence to screening schedule. J Clin Oncol 2013;31(1):49-57.
25. Rosenthal A, Fraser L, Philpott S, et al. Final results of 4-monthly screening in the UK
Familial Ovarian Cancer Screening Study (UKFOCSS Phase 2). ASCO 2013. Abstract#5507^.
26. Hampel H, Frankel W, Panescu J, et al. Screening for Lynch syndrome (hereditary
nonpolyposis colorectal cancer) among endometrial cancer patients. Cancer Res
2006;66(15):7810-7.
27. Ferguson S. Screening for Lynch syndrome in unselected women with endometrial cancer.
ASCO 2013. Abstract#5508.
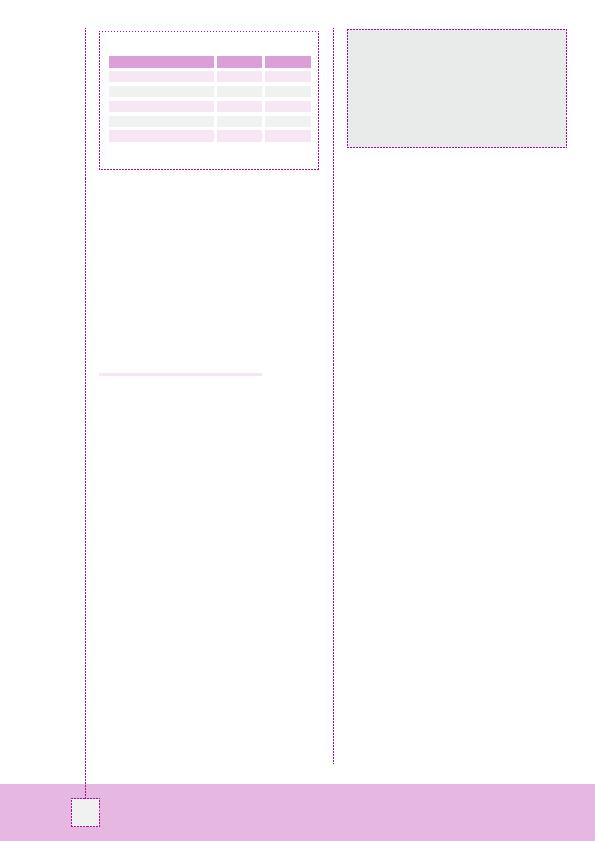
Tableau: Indices de performance du dépistage intensif.
Characteristic
Value (%)
95% CI
Sensitivity (occult true pos.)
100.0
73.5-100
Sensitivity (occult false neg.)
75.0
47.6-92.7
Specificity (occult n/a)
96.1
95.2-97.0
PPV (occult false neg.)
13.0*
6.9-21.7
NPV (occult false neg.)
99.7
99.3-99.9
* Compared with 25% in phase I
«
Ce n'est pas tant le rapprochement des dosages du CA125
que le strict respect du protocole (fût-il annuel) qui a permis la
meilleure réduction du risque. Quant à la conclusion de Sarah
Ferguson, il faut encore la confronter à la réalité économique
en y incluant les conséquences familiales. Et ce calcul semble
positif en faveur de l'immunohistochimie ciblée, au minimum
chez les femmes de moins de 60 ans.»
Michael Friedlander (Sidney)