8
GUNAIKEIA
VOL 18 Nr 9
2013
In geval van ascites moet het ascitesvocht worden onder-
zocht (20).
Behandeling
Men wil een zo weinig mogelijk mutilerende behandeling,
maar er wordt vaak gekozen voor een radicale chirurgie
(
Figuur 2) die gepaard kan gaan met meer morbiditeit (2,
5-7). Hierbij kan zeer veel bloedverlies optreden en per- en
postoperatieve monitoring is zeker noodzakelijk (2). Men zal
echter minder radicaal opereren bij een nog aanwezige kin-
derwens of wanneer hoge morbiditeit te verwachten is (2).
Gelukkig is de aanwezigheid van de tumor zelf niet dodelijk
en daarom kan men zich veroorloven om slechts een incom-
plete resectie te bewerkstelligen. Bij deze patiënten is lange-
termijnfollow-up en een brede resectie van lokaal herval zeer
belangrijk (21).
Wanneer de resectie onvolledig is of wanneer er recidieven
ontstaan, wordt er geopteerd voor hormoontherapie. Hier-
voor dient de tumor hormoongevoelig te zijn. Men zal hierbij
kiezen voor een GnrH-agonist, tamoxifen of raloxifen. Ze
kunnen dienen om de tumor te verkleinen en zo een com-
plete resectie van grote tumoren mogelijk te maken (2, 7).
recent onderzoek wijst uit dat er geen voordeel is om de
tumor te reseceren met een wijdere marge. Er is ongeveer
evenveel herval beschreven bij patiënten waarbij de snijrand
negatief was en bij patiënten waarbij de snijrand positief
was (5). Het recidief kan een paar maanden tot 20 jaar na
de operatie plaatsvinden (7). Chemotherapie en radiotherapie
worden niet aanbevolen. Chemo-embolisatie kan eventueel
nuttig zijn om de tumor te laten slinken en zo een comple-
tere resectie mogelijk te maken (8). Een langetermijnfollow-
up en monitoring is nodig gezien de hoge recurrentiegraad
(30-72%), ook al zijn de snijranden negatief (2, 5). Periodiek
klinisch onderzoek volstaat niet om herval tijdig te diagnos-
ticeren. Beeldvorming zoals MrI zal ervoor zorgen dat herval
vroeg ontdekt wordt (7).
Besluit
AAM is een zeldzame myxoïde mesenchymale tumor die
voornamelijk voorkomt in het pelvis en het perineum van
vrouwen in de reproductieve periode. Meestal metastaseert
hij niet. De tumor kan de nabijgelegen structuren infiltreren,
maar zal voornamelijk de structuren verdringen. Een karak-
teristieke eigenschap van AAM is de neiging op lokaal herval.
Daarom is efficiënte, radicale behandeling met volledige re-
sectie en hormoontherapie (in geval van een hormoondepen-
dente tumor) nodig. Intensieve opvolging is nodig gezien her-
val een paar maanden tot 20 jaar na de operatie plaatsvindt.
Gezien de aandoening vaak fout gediagnosticeerd wordt,
moet men extra waakzaam zijn wanneer een vulvaire massa
zich presenteert. Men moet verder onderzoek verrichten naar
de rol van CD44, CD34, HMGI-C als tumormarkers. Er is nood
aan het opstellen van richtlijnen voor de behandeling.
Referenties
1.
Steeper tA, rosai J. Aggressive angiomyxoma of the female pelvis and perineum. report
of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am J Surg Pathol
1983;7(5):463-75. PubMed PMID: 6684403. Epub 1983/07/01. eng.
2.
Dierickx I, Deraedt K, Poppe W, Verguts J. Aggressive angiomyxoma of the vulva: a case
report and review of literature. Arch Gynecol Obstet 2008;277(6):483-7. PubMed PMID:
18214507.
3.
Barmon D, Kataki AC, Sharma JD, Bordoloi J. Aggressive angiomyxoma of the vulva. Jour-
nal of mid-life health 2012;3(1):47-9. PubMed PMID: 22923982. Pubmed Central PMCID:
PMC3425151. Epub 2012/08/28. eng.
4.
Geng J, Cao B, Wang l. Aggressive angiomyxoma: an unusual presentation. Korean
journal of radiology: official journal of the Korean radiological Society 2012;13(1):90-3.
PubMed PMID: 22247641. Pubmed Central PMCID: PMC3253408. Epub 2012/01/17. eng.
5.
Chan YM, Hon E, Ngai SW, Ng tY, Wong lC. Aggressive angiomyxoma in females: is radical
resection the only option? Acta Obstet Gynecol Scand 2000;79(3):216-20. PubMed PMID:
10716303. Epub 2000/03/15. eng.
6.
Ichinokawa Y, Sadamasa H, Hiruma M, et al. Case of aggressive angiomyxoma of the
vulva. J Dermatol 2012 Mar 27. PubMed PMID: 22452584. Epub 2012/03/29. Eng.
7.
Bagga r, Keepanasseril A, Suri V, Nijhawan r. Aggressive angiomyxoma of the vulva in
pregnancy: a case report and review of management options. MedGenMed : Medscape
general medicine. 2007;9(1):16. PubMed PMID: 17435625. Pubmed Central PMCID:
PMC1925027. Epub 2007/04/17. eng.
8.
Han-Geurts IJ, van Geel AN, van Doorn l, den Bakker M, Eggermont AM, Verhoef C. Ag-
gressive angiomyxoma: multimodality treatments can avoid mutilating surgery. Eur J Surg
Oncol 2006;32:1217-21.
9.
Srinivasan r, Mohapatra N, Malhotra S, rao SK. Aggressive angiomyxoma presenting as a
vulval polyp. Indian journal of cancer. 2007 Apr-Jun;44(2):87-9. PubMed PMID: 17938485.
Epub 2007/10/17. eng.
10. Nucci Mr, Weremowicz S, Neskey DM, et al. Chromosomal translocation t(8;12) induces
aberrant HMGIC expression in aggressive angiomyxoma of the vulva. Genes, Chromoso-
mes Cancer 2001;32(2):172-6. PubMed PMID: 11550285. Epub 2001/09/11. eng.
11. Menzel t, Fletcher CD. the emerging role of myofibroblasts in soft tissue neoplasia. Am J
Clin Pathol 1997;107(1):2-5. PubMed PMID: 8980359. Epub 1997/01/01. eng.
12. Silverman JS, Albukerk J, tamsen A. Comparison of angiomyofibroblastoma and aggres-
sive angiomyxoma in both sexes: four cases composed of bimodal CD34 and factor XIIIa
positive dendritic cell subsets. Pathol res Pract 1997;193(10):673-82. PubMed PMID:
9505259. Epub 1997/01/01. eng.
13. Fetsch JF, laskin WB, lefkowitz M, Kindblom lG, Meis-Kindblom JM. Aggressive angio-
myxoma: a clinicopathologic study of 29 female patients. Cancer 1996;78(1):79-90.
PubMed PMID: 8646730. Epub 1996/07/01. eng.
14. Amezcua CA, Begley SJ, Mata N, Felix JC, Ballard CA. Aggressive angiomyxoma of the
female genital tract: a clinicopathologic and immunohistochemical study of 12 cases.
International journal of gynecological cancer: official journal of the International Gyneco-
logical Cancer Society 2005;15(1):140-5. PubMed PMID: 15670309.
Epub 2005/01/27. eng.
15. Bigotti G, Coli A, Gasbarri A, Castagnola D, Madonna V, Bartolazzi A. Angiomyofibroblas-
toma and aggressive angiomyxoma: two benign mesenchymal neoplasms of the female
genital tract. An immunohistochemical study. Pathol res Pract
1999;195(1):39-44. PubMed PMID: 10048093. Epub 1999/02/27. eng.
16. Nalini G, Duggal r, Neelam A, Vanita S, Arvind r. Fine needle aspiration cytology in a case
of recurrent aggressive angiomyxoma of vulva. Cytopathology: official journal of the
British Society for Clinical Cytology 2010;21(3):207-8. PubMed PMID: 19843146. Epub
2009/10/22. eng.
17. Outwater EK, Marchetto BE, Wagner BJ, Siegelman ES. Aggressive angiomyxoma: findings
on Ct and Mr imaging. AJr American journal of roentgenology 1999;172(2):435-8.
PubMed PMID: 9930798. Epub 1999/02/04. eng.
18. Havel G, Burian P, Kohrtz M, Mark J. Aggressive angiomyxoma of the vulva: an unusual,
deceptive and recurrence-prone tumour with evidence of estrogen receptor expression.
Case report. APMIS: acta pathologica, microbiologica, et immunologica Scandinavica
1994;102(3):236-40. PubMed PMID: 8185891. Epub 1994/03/01. eng.
19. Htwe M, Deppisch lM, Saint-Julien JS. Hormone-dependent, aggressive angiomyxoma
of the vulva. Obstet Gynecol 1995;86(4 Pt 2):697-9. PubMed PMID: 7675419. Epub
1995/10/01. eng.
20. Zhang P, Song K, li l, et al. Aggressive Angiomyxoma with massive ascites. Gynecologic
Oncology Case reports 2011;1(1):12-3.
21. Gungor t, Zengeroglu S, Kaleli A, Kuzey GM. Aggressive angiomyxoma of the vulva
and vagina. A common problem: misdiagnosis. Eur J Obstet Gynecol reprod Biol
2004;112(1):114-6. PubMed PMID: 14687754. Epub 2003/12/23. eng.
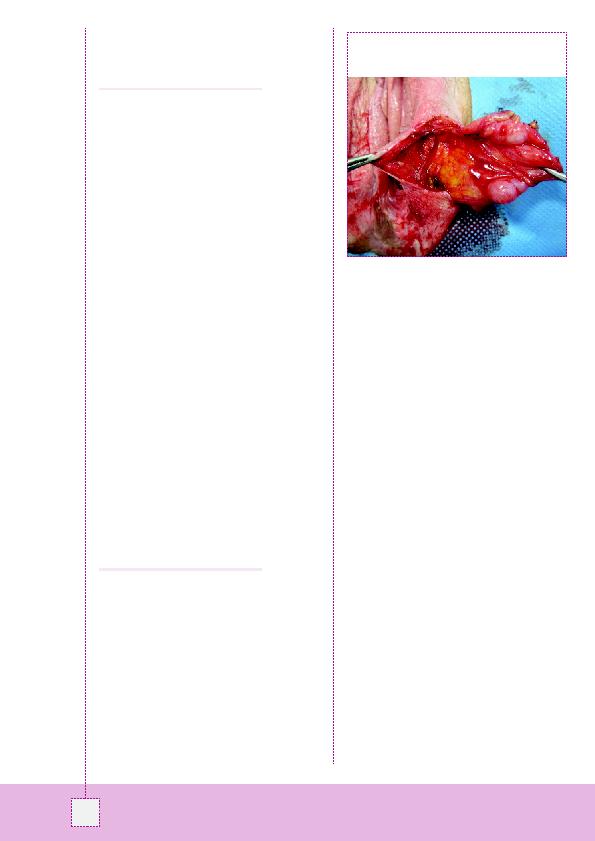
Figuur 2: De gelobde massa werd
`en bloc' verwijderd met
omliggend bindweefsel. De massa breidde paraclitoraal uit.
Microscopisch waren de resectieranden tumorvrij.